menuclose

What is the Transcatheter Aortic Valve Implantation (TAVI) Procedure?
To support optimal patient outcomes, patients with a clinical suspicion of aortic valve disease should be referred to a specialist (irrespective of symptoms) for further evaluation to aid in the planning of appropriate long-term management. The only effective treatment for severe aortic stenosis is to replace the diseased aortic valve. Medical therapy may provide temporary relief of symptoms although it does not improve outcomes. Balloon valvuloplasty may be considered as a bridge to valve replacement but is usually followed by restenosis and deterioration within 6–12 months.
The TAVI Procedure
In a TAVI procedure, a biological (tissue) valve is mounted inside a stent (a circular wire mesh). The stent is then compressed so that it can fit inside a small delivery sheath (tube). The TAVI valve is then delivered to the aortic valve, the stent is expanded, and the biological valve inside begins to work. In TAVI the calcified leaflets of the patient’s diseased aortic valve are not removed; instead, they are pushed to the side when the stent expands and help to lock the stent in place.
There are multiple ways of delivering the TAVI valve to the aortic valve position including:
- Transfemoral – The delivery sheath is inserted into the femoral artery in the patient’s groin, and the TAVI valve travels upwards through the artery to the aortic valve.
- Transapical – A 5-10cm horizontal incision is made on the left side of the chest below the nipple line, which provides direct access to the heart. The delivery sheath is then inserted in the apex of the heart and the TAVI valve inserted.
- Transaortic – A small incision at the top of the sternum (breast bone) is made and that the delivery sheath is inserted into the aorta (the large blood vessel that the aortic valve is in).1
TAVI Procedure: Step-By-Step
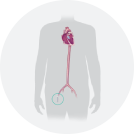 Step 1 of 4
Step 1 of 4
A small incision is made into the Femoral Artery in your groin. Then a sheath is introduced into the artery and a long radiopaque wire is inserted into the sheath, this will sit just superior to the aorta. This allows the introduction of a larger sheath which will deliver the new aortic valve.
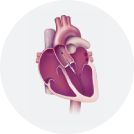 Step 2 of 4
Step 2 of 4
The new aortic valve is placed on a delivery sheath, compressed and made small enough to be delivered through the catheters already in the femoral artery.
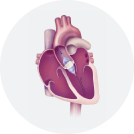 Step 3 of 4
Step 3 of 4
The radiopaque guidewire is introduced into the heart, and the delivery sheath is placed in position within the diseased native aortic valve. A balloon is inflated to increase the size of the native valve, and then a new valve is deployed within the old diseased valve. The catheters are then removed from the femoral artery.
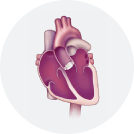 Step 4 of 4
Step 4 of 4
The new valve will begin working as soon as the catheters and wires are removed from the heart. Echocardiography testing during the procedure ensures that your new valve is functioning as effectively as it should. The femoral artery may be closed to prevent bruising and bleeding at the site.